
June is Alzheimer’s and Brain Awareness Month, raising global awareness about brain health, fighting cognitive decline, and supporting those living with Alzheimer’s and dementia.
Alzheimer’s and Brain Awareness Month is an opportunity for us to highlight the clinical, pathological, and social impact of Alzheimer’s disease, the most common cause of dementia in the developed world. Alzheimer’s disease is characterized by progressive cognitive decline, with hallmark pathological features including extracellular amyloid-beta plaques and intracellular neurofibrillary tangles composed of hyperphosphorylated tau protein, leading to neuronal dysfunction and cerebral atrophy.
The disease typically affects the hippocampus, temporal, and parietal lobes, sparing primary motor and sensory cortex.
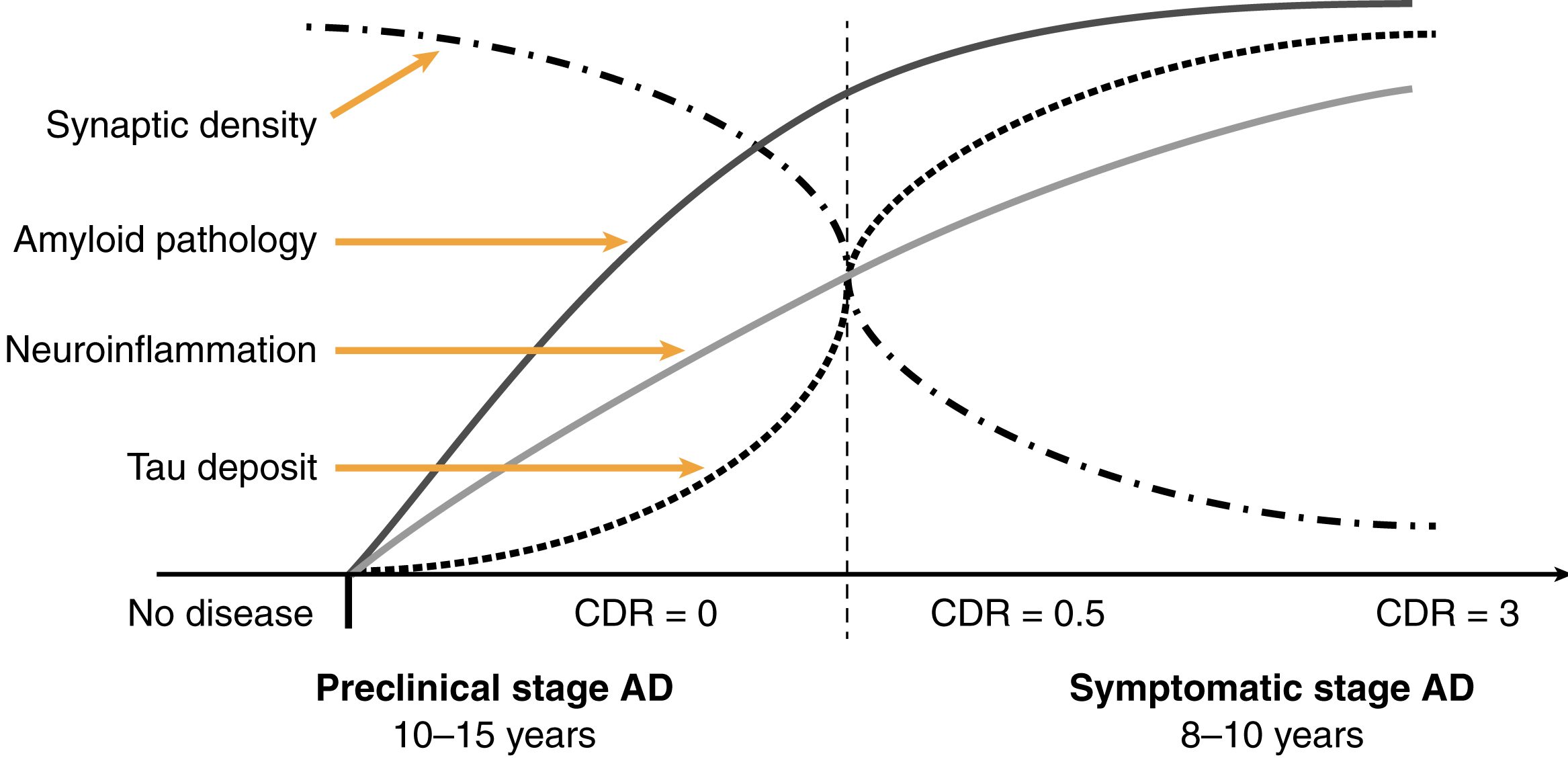
Pathological Timeline and Pathological Features
Alzheimer’s disease pathology develops over years before symptoms appear, with amyloid accumulation preceding tau pathology and synaptic loss. As the disease progresses, patients experience increasing dependence on carers and ultimately require institutional care, with death often resulting from complications such as pneumonia.
- Alzheimer’s disease is defined by the presence of extracellular amyloid-beta plaques and intracellular neurofibrillary tangles composed of hyperphosphorylated tau protein.
- Amyloid plaques are most common in the hippocampus, entorhinal cortex, and amygdala, and are associated with cognitive decline.
- Neurofibrillary tangles are found in the cytoplasm of neurons and may persist after neuronal death as ‘ghost tangles.
- Amyloid can also be deposited in cerebral blood vessels, leading to cerebral amyloid angiopathy.
- There is widespread neuronal and synaptic loss, especially in the hippocampus and medial temporal lobe, with degeneration of cholinergic neurons in Meynert’s nucleus.
Clinical Presentation and Progression
- Alzheimer’s disease presents with progressive episodic memory loss, often accompanied by apraxia, aphasia, agnosia, and impaired executive function
- Early features include difficulty with word finding, planning, and visuospatial tasks; personality and social behaviour are relatively preserved until late stages
- Patients may become repetitive, misplace items, and experience topographical disorientation
- Late features include myoclonus, seizures, agitation, delusions, and eventual dependence on carers for all activities of daily living
- Death is often due to complications of immobility, such as pneumonia
Risk Factors and Genetics
- Advancing age is the strongest risk factor for Alzheimer’s disease
- Genetic predisposition includes the APOE e4 allele, which increases risk, and the APOE e2 allele, which is protective
- Familial cases are associated with mutations in APP, PSEN1, and PSEN2 genes
- Low educational attainment, low social engagement, stroke, depression, and heavy alcohol consumption are additional risk factors
Diagnosis and Management
- Diagnosis is based on characteristic clinical features and supported by imaging (CT/MRI showing cerebral atrophy, especially in temporal lobes)
- Definitive diagnosis requires histopathology, but clinical diagnosis is usually accurate
- Management includes acetylcholinesterase inhibitors (donepezil, galantamine, rivastigmine) for mild-to-moderate disease, and memantine for moderate-to-severe disease
- Emerging disease-modifying therapies include anti-amyloid-beta monoclonal antibodies, which require monitoring for amyloid-related imaging abnormalities
Related Resources
- Osmosis Video, Alzheimer’s Disease-video explanation
- Osmosis Video, Alzheimer’s Disease: Clinical Sciences
- “Medicine in a day: Revision Notes” Book, Chapter 13 “Neurology in an Hour – Cognitive Neurology: Alzheimer’s Disease” available on ClinicalKey Student
- “Crash Course Neurology & Ophthalmology” Book, Chapter 21 “Dementia – Primary neurodegenerative dementias” available on ClinicalKey Student
- “Clinical Neuroscience” Book, Chapter 12 “Dementia” available on ClinicalKey Student
- “Psychiatry: An Illustrated Colour Text” Book, Chapter 39 “Dementia Diagnosis, Alzheimer’s Disease” available on ClinicalKey Student
- “The Nervous System” Book, Chapter 14 “Dementia” available on ClinicalKey Student
Content developed using ClinicalKey Student, StudyFinder AI, the new AI enhancement designed to help you find what you need faster!
Click here to check if you have StudyFinder AI access via your institution
Leave a Reply